-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
- Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
December 2025
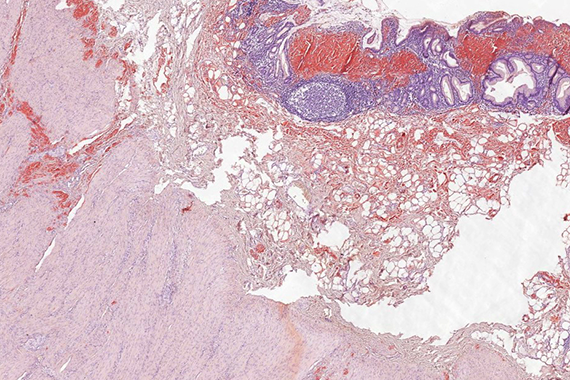
Biopsy and resection of stomach from a 45-year-old male with suspected gastric cancer.

Diagnosis
Localized gastric amyloidosis.
Comment
A 45-year-old male patient was admitted for upper gastrointestinal endoscopy due to progressive weight loss and fatigue.
Endoscopy revealed diffuse infiltration of gastric wall along the lesser curvature. The mucosa was pale, thickened, friable and easily bleeding. Based upon endoscopic findings a biopsy of gastric mucosa was performed with the suspicion for infiltrative gastric cancer.
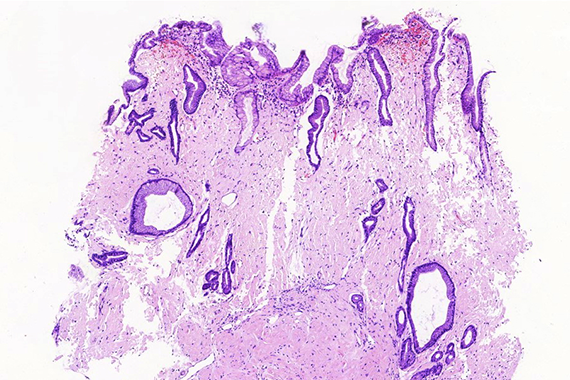
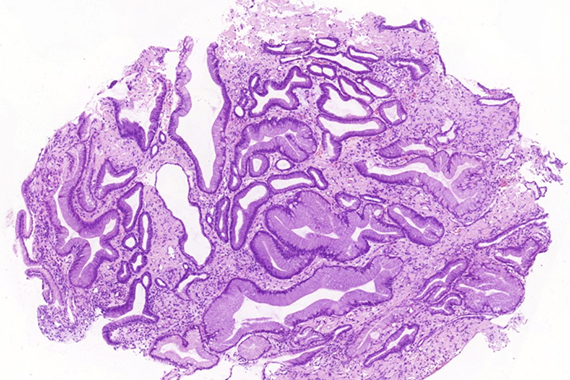
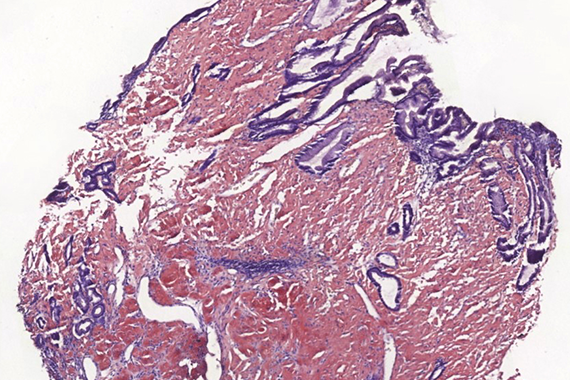
Histologically, lamina propria of gastric mucosa was expanded with amorphous paucicellular stromal deposits with cracking artifacts (Panels A and B). These depositions stained red with Congo Red stain (Panel C) and demonstrated characteristic apple-green birefringence in polarized light (Panel D). No malignancy was observed. Consequently, the final diagnosis was gastric amyloidosis.
On further thorough clinical examination no other foci of amyloid deposits were found, no signs of underlying systemic hematological disorder were revealed, and subtyping of amyloid deposits in gastric biopsy (performed in another institution) proved them to be of an AL-type.
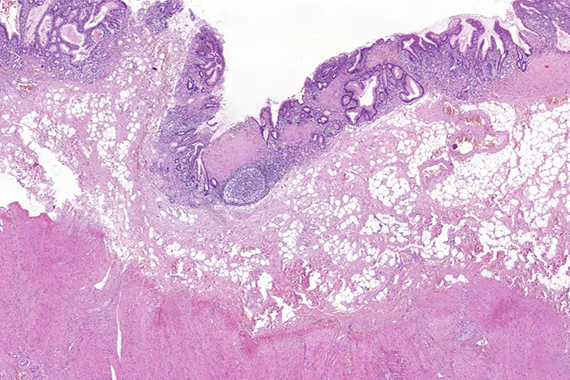
Due to recurrent gastrointestinal bleeding and significant involvement of the stomach with amyloidosis, a distal resection of stomach was performed. Histological findings (Panel E) in the resection specimen, including Congo Red stain (Panel F) were similar to those described in the pre-operative biopsy.
For further reading
- Liu XM, Di LJ, Zhu JX, Wu XL, Li HP, Wu HC, Tuo BG. Localized primary gastric amyloidosis: Three case reports. World J Clin Cases. 2020 Oct 6;8(19):4667-4675. doi: 10.12998/wjcc.v8.i19.4667. PMID: 33083432.
- Lin XY, Pan D, Sang LX, Chang B. Primary localized gastric amyloidosis: A scoping review of the literature from clinical presentations to prognosis. World J Gastroenterol. 2021 Mar 28;27(12):1132-1148. doi: 10.3748/wjg.v27.i12.1132. PMID: 33828390.
- Dahiya DS, Kichloo A, Singh J, Albosta M, Wani F. Gastrointestinal amyloidosis: A focused review. World J Gastrointest Endosc. 2021 Jan 16;13(1):1-12. doi: 10.4253/wjge.v13.i1.1. PMID: 33520102.
Presented by
Dr. Hanna Lapsar, Kyiv, Ukraine.
