-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
- Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
January 2025
Full thickness resection (FTRD-specimen) from the transverse colon with a polypoid lesion.
Diagnosis
Lifting agent granuloma.
Comment
A 69-year-old male underwent polypectomy in the transverse colon. Histological examination of the removed polyp revealed tubular adenoma with high grade dysplasia. Years later, another colonoscopy was performed and a new polypoid lesion was noted at the polypectomy site, macroscopically suspicious for recurrence of adenoma or a new neoplasm. The lesion was completely excised endoscopically using the FTRD (full thickness resection device)-technique.
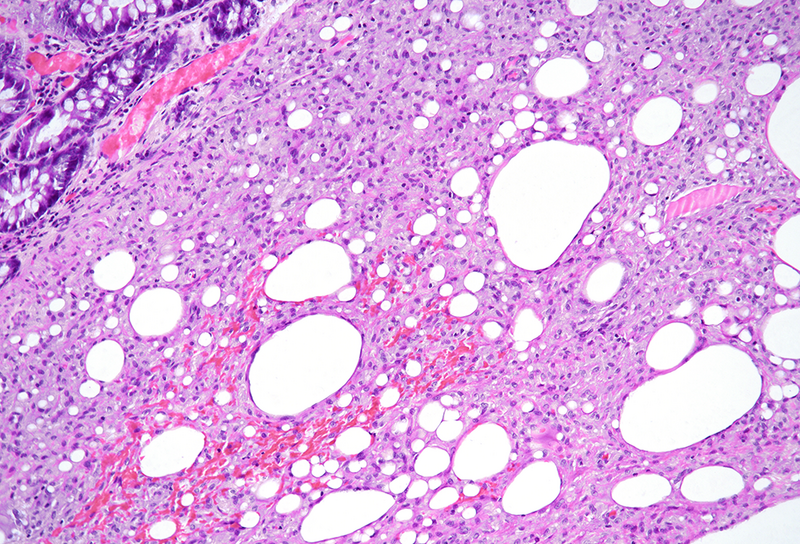
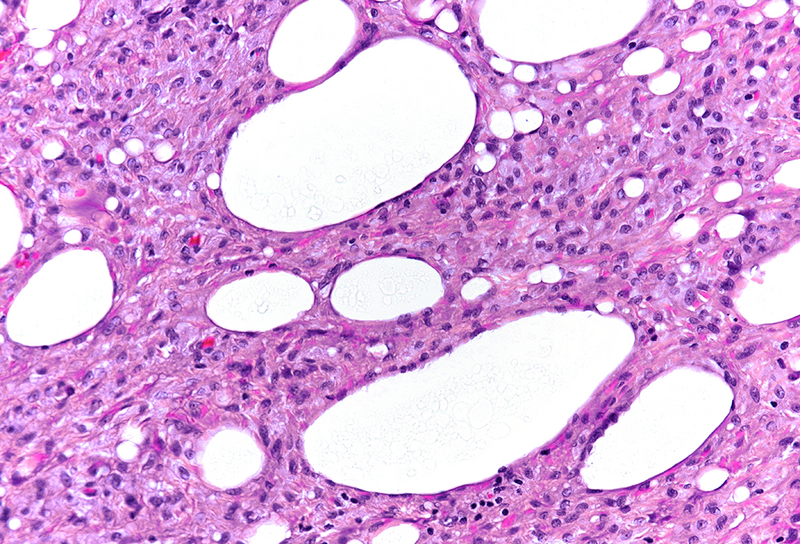
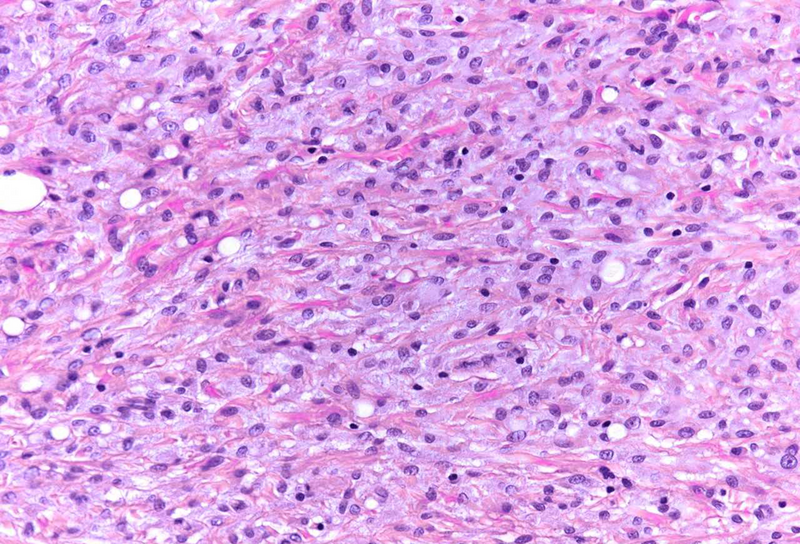
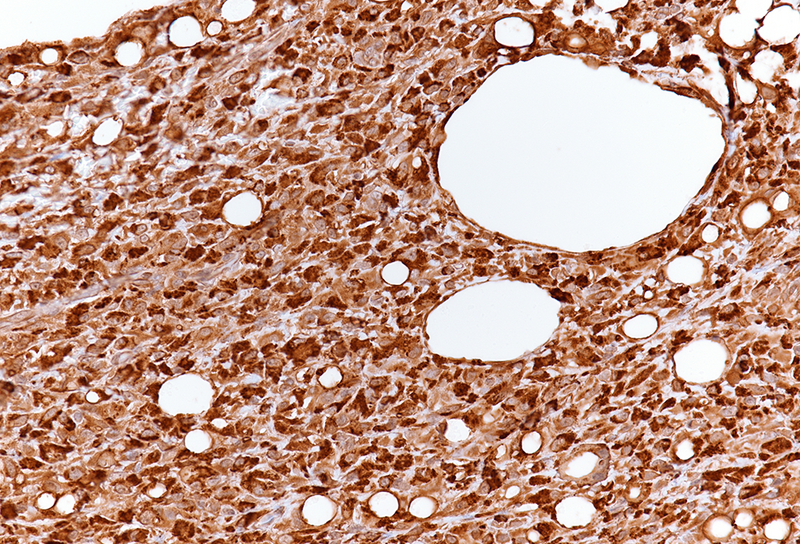
The resection specimen contained superficial remnants of the previously excised tubular adenoma (not shown). Close to the neoplastic glands, however within the submucosa, nodular aggregates of histiocytes were found (Panel A), that included vacuoles of varying size; these vacuoles were mainly empty, except for few tiny droplets of pale fluid or substance (Panels B and C). A CD68 immunostain confirmed histiocytic cell origin (Panel D). Pankeratin staining was negative within the lesion. No atypia was observed, and no eosinophils were present. The histological findings in combination with a history of polypectomy at the same site were consistent with the diagnosis of a “lifting agent granuloma”.
Lifting agents are used in endoscopic mucosal resections and submucosal dissection of neoplasms in the upper and lower GI tract to elevate the mucosa from the muscularis propria. Non-saline solutions often remain present in the tissue surrounding the polypectomy site and might cause local inflammation and foreign body reaction. Occasionally, remaining lifting agents and associated granuloma can present as mass-forming lesions and mimic polypoid neoplasms macroscopically and radiologically. Depending on the type of injection solution and the associated microscopic changes, lifting agents can histologically be mistaken for mucin, amyloid or pulse material. Clinicians and pathologists should be aware of this phenomenon in order to avoid misdiagnosis and overtreatment.
For further reading
- Ibarra-Arzamendia PN, Hanly MG. Histopathological Findings Related to ORISE™ Injectable Submucosa Lifting Agent Used in the Endoscopic Mucosal Resection of Bowel Neoplasms: A Review of Three Cases. Case Rep Pathol. 2020 Jan 29;2020:6918093. doi: 10.1155/2020/6918093.
- Westbrook LM, Henn PA, Cornish TC. Lifting Agent Granuloma: Histologic Findings Following Use of ORISE Gel for Endoscopic Resections in the Gastrointestinal Tract. Am J Clin Pathol. 2020; 153: 630-8.
- Mendelson NL, Elliott KR, Evans KE, Frisch NK, Abu Alfa AK. Lifting agent granuloma presenting as a colonic mass mimicking cancer: a report of three cases. AME Case Rep. 2023 Jan 6;7:6.
Presented by
Dr. Johanna Köhler, Linköping, Sweden, and Dr. Cord Langner, Graz, Austria.
