-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
- Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
July 2025
Oesophageal biopsies from a 67-year-old male patient with dysphagia.


Diagnosis
Lymphocytic oesophagitis.
Comment
A 67-year-old male patient underwent upper-GI endoscopy for dysphagia and odynophagia. The endoscopic findings were unremarkable, and routine biopsies were taken.
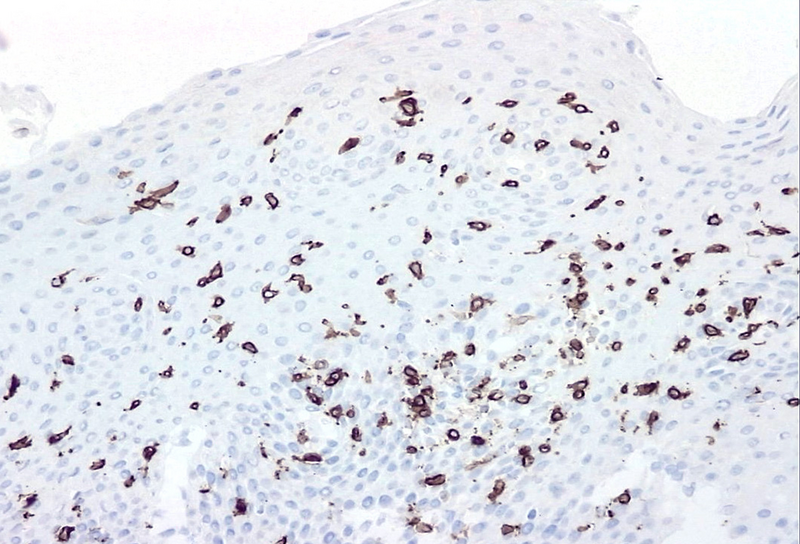
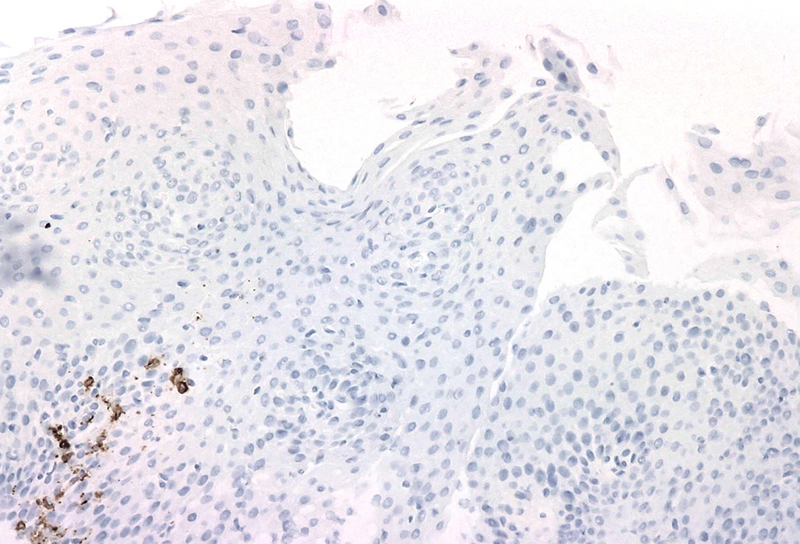
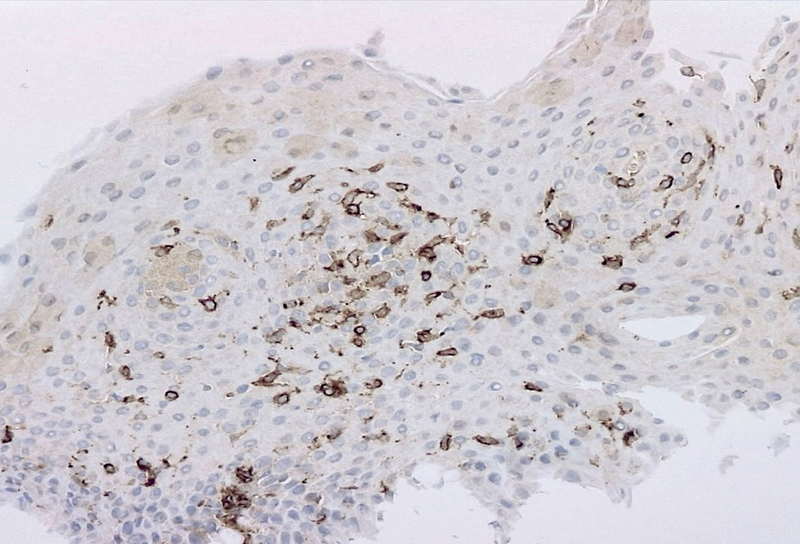
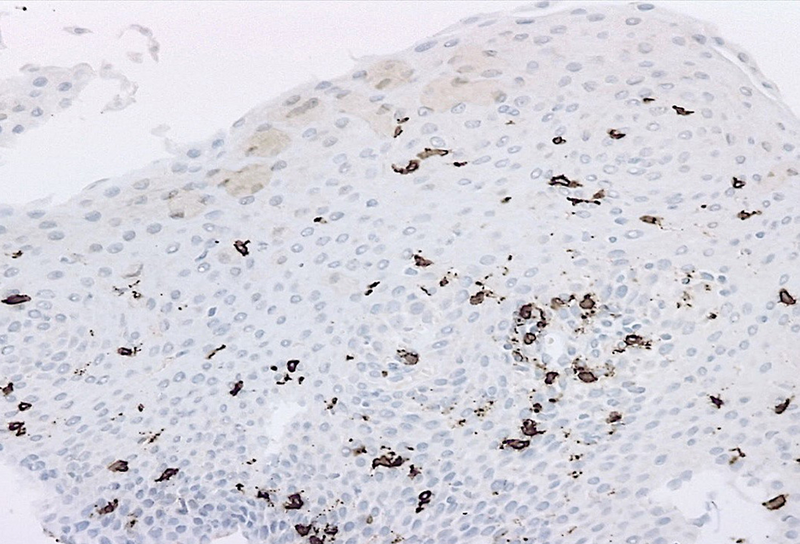
Microscopic examination revealed oesophageal squamous mucosa with an increased number of intraepithelial lymphocytes predominantly clustered around papillae, rare to absent granulocytes, intercellular oedema known as spongiosis and basal cell hyperplasia (Panels A and B). Most of the lymphocytes in the infiltrate were T cells CD3+ (Panel C). CD20 stain shows rare B cells (Panel D). CD4+ T cells outnumber CD8+ T cells (Panels E and F).
Lymphocytic oesophagitis is a poorly defined clinicopathologic condition. Because different clinical diagnoses can present with an increase in intraepithelial lymphocytes, many pathologists prefer the term "lymphocytic oesophagitis pattern of injury" as a diagnostic descriptor. The prevalence of this entity in the literature has increased in recent years, possibly due to the volume of oesophageal biopsies taken during oesophagoscopy and due to increasing recognition of the condition by pathologists and clinicians. Lymphocytic oesophagitis may be seen in children with Crohn’s disease, and in adults, it shows a predilection for middle-aged women with immune-mediated disorders, achalasia, and other motility disorders.
Endoscopic findings on lymphocytic oesophagitis may resemble those seen in eosinophilic oesophagitis, such as oesophageal rings, erythema, white plaques, furrows, and strictures. However, endoscopy is normal in about 20% of cases (“microscopic oesophagitis”). Thus, in patients with dysphagia and normal endoscopy, step biopsies from all areas of the oesophagus should be taken to arrive at definitive diagnosis.
There is no standard number of intraepithelial lymphocytes required for diagnosis and studies have included various cut-off values, ranging from 20 to 50 lymphocytes/HPF. A recently published consensus recommendation by an international expert panel suggests 40 lymphocytes per HPF as cut-off value, following Rubio’s initial criteria for diagnosis. Lymphocytic oesophagitis varies in the prevalence of CD4+ or CD8+ T cells. The predominance of CD4+ intraepithelial lymphocytes appears to be associated with dysphagia, primary oesophageal motility abnormalities and prominent spongiosis.
It has to be kept in mind, however, that the by far most common cause of lymphocyte-rich inflammation within the oesophagus is candida infection. Therefore, special stains are inevitable, ideally performed on endoscopic smears / brushings.
Although the condition tends to follow a benign course, persistent symptoms can impact quality of life, and treatment is primarily symptomatic management, such as proton pump inhibitors, swallowed topical steroids, endoscopic dilation, with no standardized protocol established yet.
For further reading
- Rubio CA, Sjodahl K, Lagergren J. Lymphocytic esophagitis: a histologic subset of chronic esophagitis. Am J Clin Pathol. 2006; 125(3): 432-437
- Martin IW, Atkinson AE, Liu X, Suriawinata AA, Lefferts JA, Lisovsky M.
- Mucosal inflammation in Candida esophagitis has distinctive features that may be helpful diagnostically. Mod Pathol. 2018; 31(11): 1653-1660
- Haque S, Genta RM. Lymphocytic oesophagitis: clinicopathological aspects of an emerging condition. Gut. 2012; 61 (8) :1108-1114
- Xue Y, Suriawinata A, Liu X, Li Z, Gabbard S, Rothstein R, Lacy B, Lisovsky M. Lymphocytic Esophagitis With CD4 T-cell-predominant Intraepithelial Lymphocytes and Primary Esophageal Motility Abnormalities: A Potential Novel Clinicopathologic Entity. Am J Surg Pathol. 2015; 39 (11): 1558-1567
- Coady LC, Sheahan K, Brown IS, Carneiro F, Gill AJ, Kumarasinghe P, Kushima R, Lauwers GY, Pai RK, Shepherd NA, Slavik T, Srivastava A, Langner C. Esophageal lymphocytosis: exploring the knowns and unknowns of this pattern of esophageal injury. Expert Rev Gastroenterol Hepatol. 2024; 18: 529-539
Presented by
Dr. Andreea-Iuliana Praf, Dr. Andrei Haidar, and Dr. Gabriel Becheanu, Bucharest, Romania.
