-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
- Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
March 2026
Colon biopsies in a 87 year-old female with chronic watery diarrhea.
Diagnosis
Collagenous colitis with giant cells.
Comment
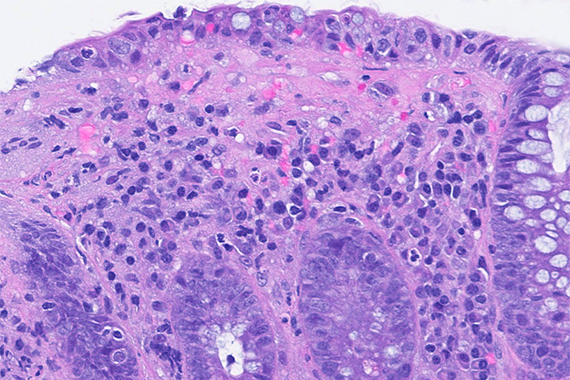
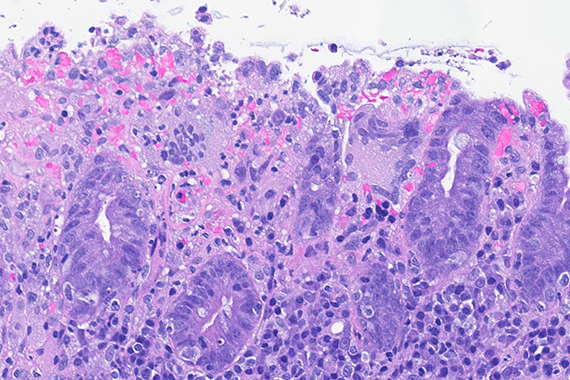
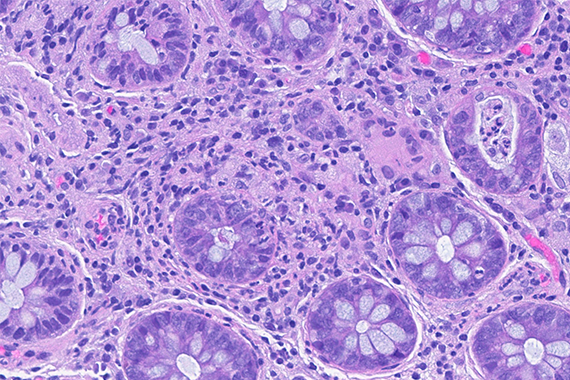
An 87-year-old woman presented with chronic, non-bloody, watery diarrhea and underwent colonoscopy, which revealed no endoscopic abnormalities. Biopsies were taken.
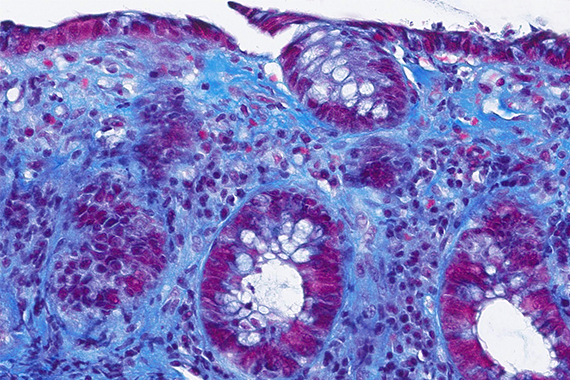
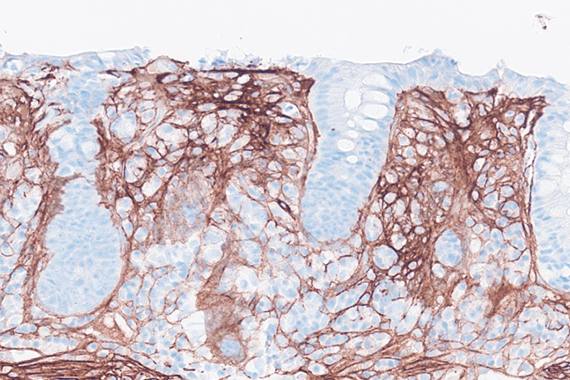
Histology of several colonic sites showed a thickened subepithelial collagen band (>10 μm), predominantly beneath the superficial epithelium but also surrounding the crypts (Panel A). Surface epithelial injury was also observed, with focal mucin depletion and detachment of superficial epithelial cells (Panel B). Lamina propria showed increased cellularity, with lymphocytic and plasmocytic infiltration, along with numerous giant cells (Panel C). There was no crypt architectural distortion. The collagen deposition was highlighted by Masson’s trichrome stain (Panel D) and strongly by tenascin immunohistochemistry (Panel E).
Collagenous colitis, together with lymphocytic colitis, falls under the clinicopathological umbrella term microscopic colitis. It predominantly affects older adults and shows a female predominance, particularly in collagenous colitis. The main symptom is chronic, non-bloody, watery diarrhea, while endoscopic findings are typically unremarkable. The pathogenesis is not yet fully understood but is considered multifactorial, likely involving dysregulated immune responses to luminal antigens, impaired intestinal barrier function and alterations in myofibroblast activity.
Due to its patchy distribution, multiple biopsies should be taken when microscopic colitis is suspected.
Histological variants of both collagenous and lymphocytic colitis have been described, including collagenous colitis with giant cells. In this variant, multinucleated giant cells are abundant and scattered throughout the lamina propria, with no apparent prognostic value.
For further reading
- Libbrecht L, Croes R, Ectors N, Staels F, Geboes K. Microscopic colitis with giant cells. Histopathology. 2002;40(4):335-338.
- Chang F, Deere H, Vu C. Atypical forms of microscopic colitis: morphological features and review of the literature. Adv Anat Pathol. 2005 Jul;12(4):203-211.
- Münch A, Langner C. Microscopic colitis: clinical and pathologic perspectives. Clin Gastroenterol Hepatol. 2015;13(2):228–236.
- Langner C, Aust D, Ensari A, Villanacci V, Becheanu G, Miehlke S, et al.; Working Group of Digestive Diseases of the European Society of Pathology (ESP) and the European Microscopic Colitis Group (EMCG). Histology of microscopic colitis - review with a practical approach for pathologists. Histopathology. 2015;66(5):613–626.
- De Petris G, Chen L. Evolution of microscopic colitis to giant cell colitis without significant intraepithelial lymphocytosis or thickened collagen plate. Int J Surg Pathol. 2015;23(3):225-229.
Presented by
Dr. Ana Lucia Alves, Coimbra, Portugal, and Dr. Cord Langner, Graz, Austria.
