-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
- Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
February 2024
Colon tumour biopsy in an 86-year-old female.
Diagnosis
Poorly differentiated adenocarcinoma of the colon with a nuclear dot-like MLH1 staining artifact.
Comment
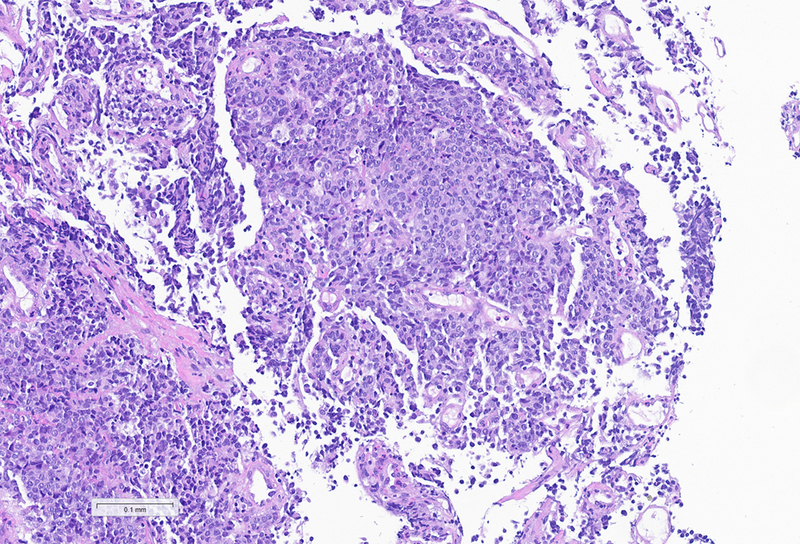
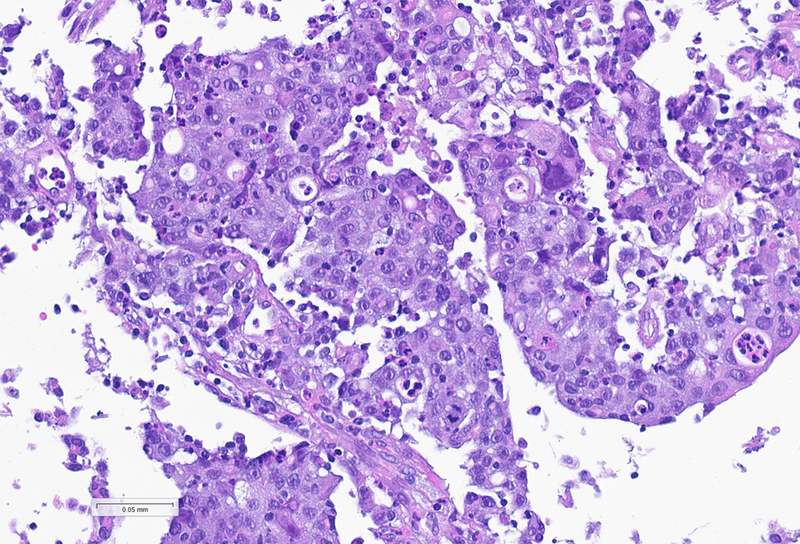
An 86-year-old female patient underwent colonoscopy, during which a mass lesion was identified in the left colonic flexure. Biopsies were taken. Histologically, the tumour proved to be a poorly differentiated cancer with solid architecture, marked cellular and nuclear pleomorphism and increased mitotic activity (Panels A and B). The tumour was positive for pancytokeratin, CDX2 and MUC2 (in the cytoplasm of individual cells), confirming the lesion to be a poorly differentiated adenocarcinoma of the colon. It was negative for neuroendocrine markers (chromogranin A, synaptophysin and CD56) as well as for LCA, desmin, S100, WT1, TTF1 and CD99. INI1 and SMARCA4 expression were retained.
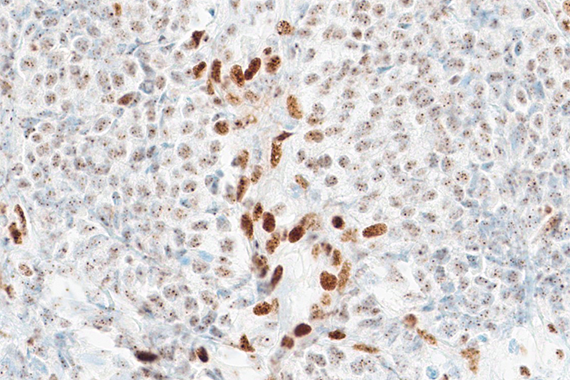
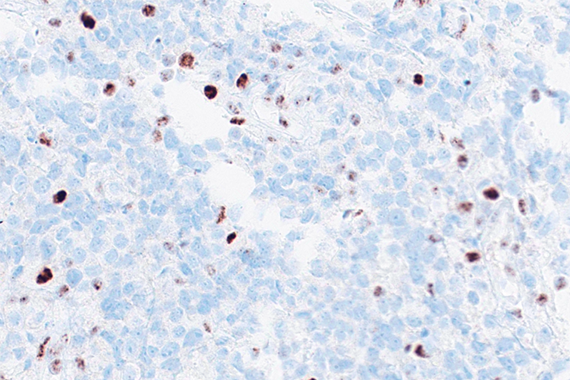
Immunohistochemistry for mismatch repair proteins showed a weak nuclear dot-like staining pattern for MLH1 in tumour cells (Panel C), while PMS2 was completely negative (Panel D). MSH2 and MSH6 were diffusely positive.
The expected positive pattern of mismatch repair proteins on immunohistochemistry is strong nuclear staining in tumour cells. However, several exceptions have increasingly been recognised, as these stains are now routinely performed in all newly diagnosed adenocarcinomas of the colon (as well as carcinomas from other sites), to rule out Lynch syndrome and identify microsatellite instability, which implies a treatment option, i.e. immunotherapy, in stage IV disease for many cancers. The nuclear dot-like pattern of MLH1 expression, as observed in this case, has been shown to be artefactual and clone-related, and does not indicate retained expression. This staining pattern represents an important diagnostic pitfall, particularly when MLH1 is used without additional PMS2 staining. Its recognition is important, as misinterpretation may lead to inadequate investigation for Lynch syndrome, and patients may not receive appropriate anti-cancer treatment.
For further reading
Dasgupta S, Ewing-Graham PC, Groenendijk FH, Stam O, Biermann KE, Doukas M, et al. Granular dot-like staining with MLH1 immunohistochemistry is a clone-dependent artefact. Pathol Res Pract. 2020;216:152581.
Shia J. The diversity of tumours with microsatellite instability: molecular mechanisms and impact. Histopathology. 2020;76(1):1–15.
Wang C, Huang Y, Huang Y, et al. Mismatch repair deficiency and microsatellite instability in colorectal carcinoma: molecular mechanisms and clinical implications. Mod Pathol. 2022;35(2):199–210
Presented by
Dr. Ana Lucia Alves, Coimbra, Portugal, and Dr. Cord Langner, Graz, Austria.
