-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
- Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
July 2026
Bile duct obstruction in an 89-year-old female.

Diagnosis
Intrabiliary Growth Type Metastasis of colorectal cancer.
Comment
An 89-year-old woman presented with jaundice due to stenosis of the common bile duct. She had prior history of high-grade adenocarcinoma of the ileocaecal valve, for which she had undergone a right hemicolectomy two years earlier. At that time, the tumour had perforated the colonic serosa and there were lymph node metastases as well as liver and ovarian metastases. Endoscopic biopsies of the bile duct stenosis were taken.
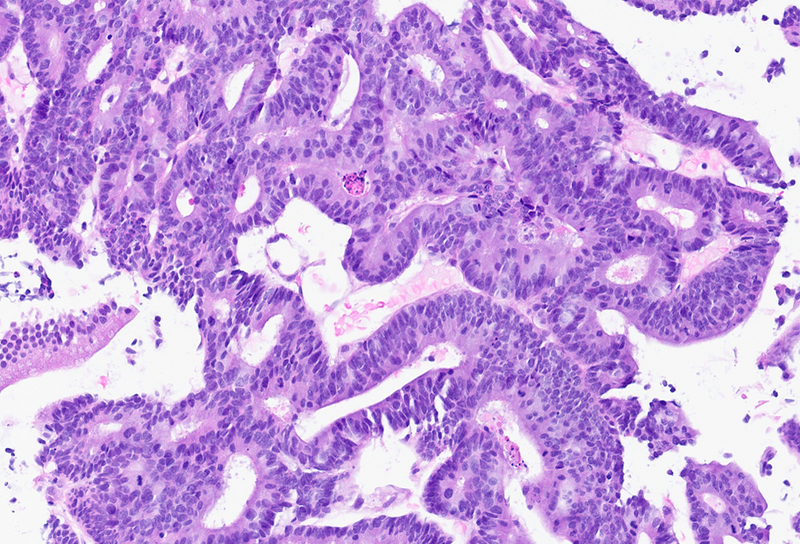
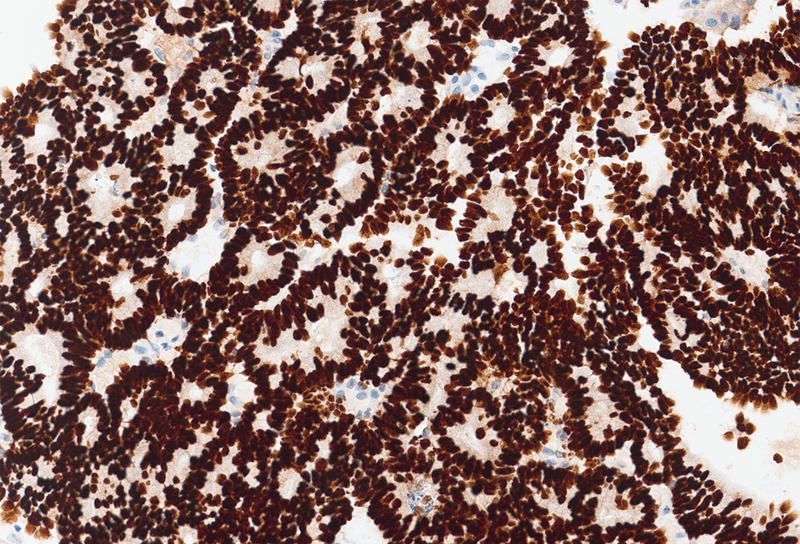
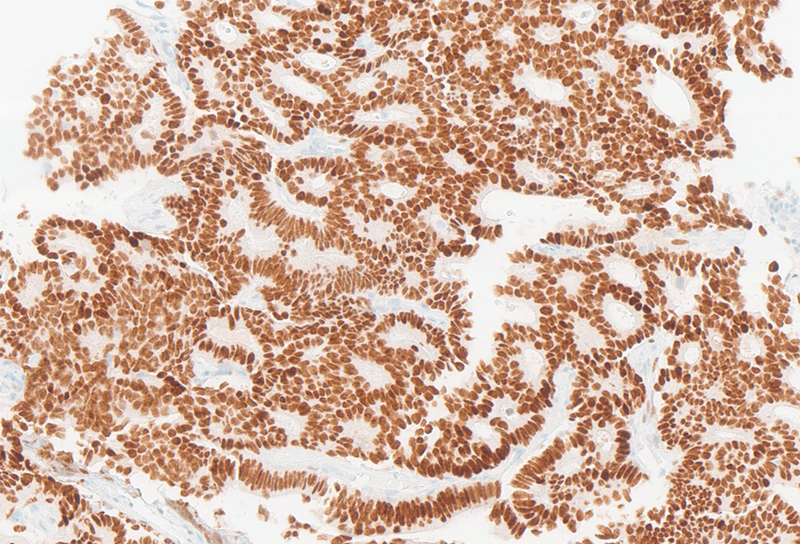
On histological examination, there was an adenocarcinoma with tubular and cribriform architecture, cellular atypia and readily identifiable mitotic activity (Panel A). Tumour cells were positive for CK20, CDX2 and SATB2 (Panels B, C and D, respectively) and negative for CK7, strongly supporting a colorectal origin (as opposed to a biliary origin). Rare fragments of normal biliary epithelium, CK7 positive and negative for all other immunomarkers, served as an internal control.
While colorectal adenocarcinoma is one of the most common malignancies worldwide, cholangiocarcinoma is a relatively rare entity.
Adenocarcinomas of the colon and rectum are known to commonly metastasize to regional lymph nodes, liver and lungs. However, metastasis to the extrahepatic biliary tree has also been reported in the literature and may be more frequent than previously thought.
Distinguishing between a primary biliary tumour and a metastasis from colorectal adenocarcinoma to the biliary tree can be challenging, as colorectal, primary biliary, or even pancreatic adenocarcinomas may be morphologically similar. Recognizing the possibility of metastasis is essential for accurate diagnosis, which has significant impact on patient management.
For further reading
Coppola S, Zucchini N, Romano F, et al. Colorectal liver metastasis with intrabiliary growth: case report and review of the literature. Int J Surg Pathol. 2014;22(3):272–279.
Strauss AT, Clayton SB, Markow M, et al. Colon cancer metastatic to the biliary tree. ACG Case Rep J. 2016;3(3):214–216.
Knowles KJ, Chen S, Herrera GA. Metastatic colonic adenocarcinoma to the extrahepatic common bile duct: the critical role of the pathologist and immunohistochemistry in guiding patient care decisions. Am J Case Rep. 2017;18:263–266.
Wright K, Mederos MA, Riahi IR, et al. Solitary synchronous biliary metastasis in colorectal adenocarcinoma. World J Oncol. 2025;16(2):227–234.
O’Leary RJ, Siegel JB, Moran RA, et al. An early-stage colon cancer develops intrabiliary growth type metastasis 7 years after curative colectomy. Am Surg. 2023;89(11):4888–4890.
Presented by
Dr. Ana Lucia Alves, Coimbra, Portugal, and Dr. Cord Langner, Graz, Austria.
