-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
- Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
June 2026
Gastric antral polypectomy in a 86-year-old female.

Diagnosis
Gastric hyperplastic polyp with intramucosal adenocarcinoma.
Comment
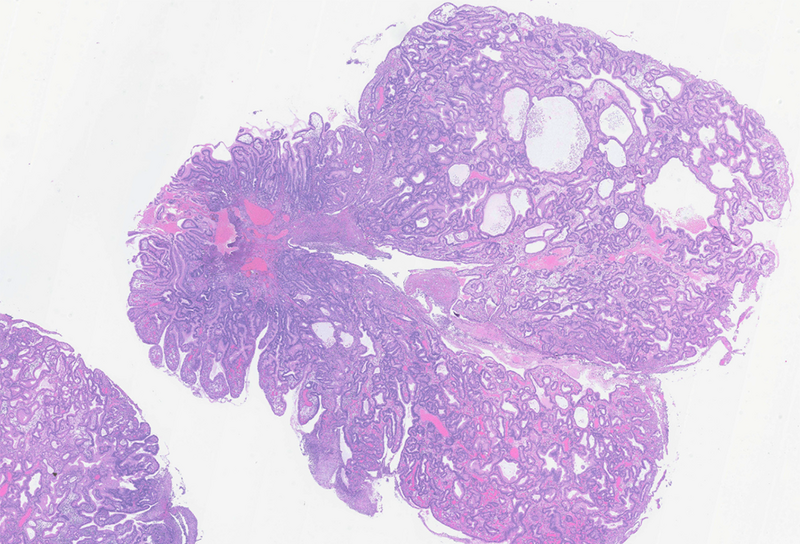
An 86-year-old female patient underwent endoscopic investigation of the upper gastrointestinal tract, during which a polyp measuring 3 cm in its largest dimension was identified in the gastric antrum. A polypectomy was performed.
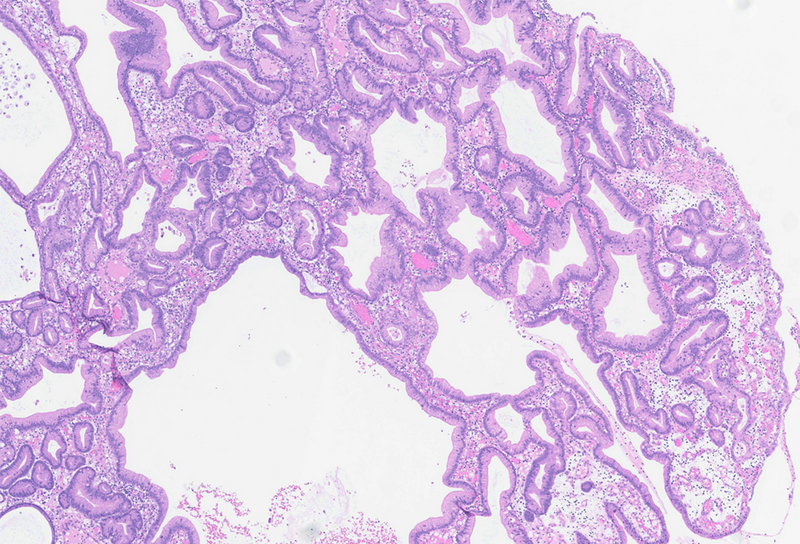
Histologically, the lesion proved to be a gastric hyperplastic polyp, composed of elongated and distorted hyperplastic foveolae, with focal erosion (Panels A and B). The glandular pits were irregular and cystically dilated (Panel C) and the surrounding stroma was edematous, containing abundant inflammatory infiltrate and scattered thin-walled vessels.
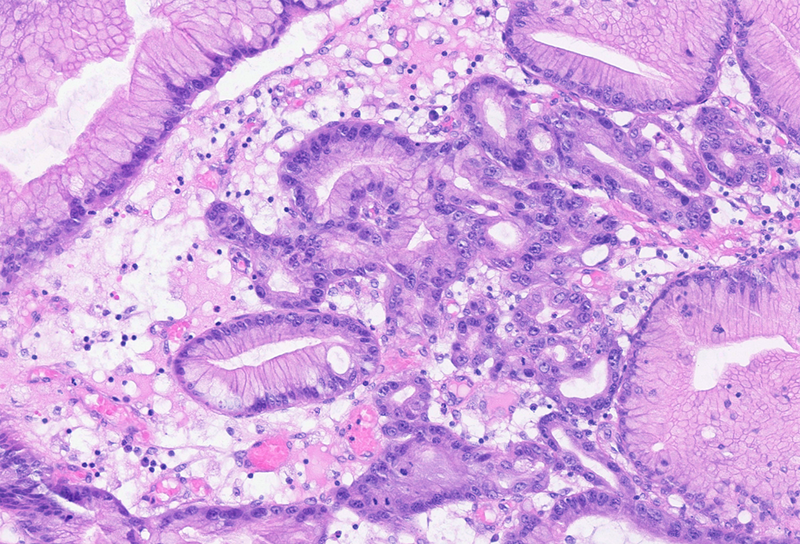
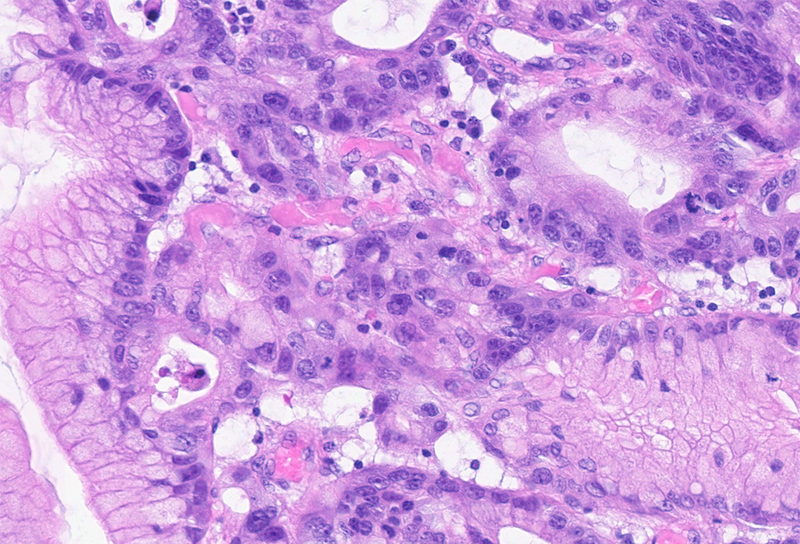
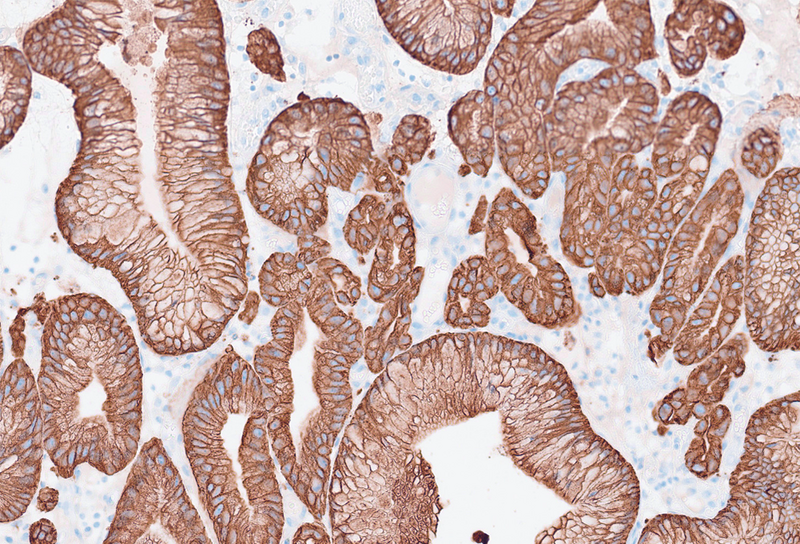
Focally, high-grade dysplasia was present, with cytologic atypia, loss of polarity, enlarged nuclei and prominent nucleoli. In these high-grade dysplastic areas, glandular crowding, a cribriform architectural pattern and small infiltrative tumour nests were also present (Panels D and E) and highlighted by pancytokeratin immunohistochemistry (Panel F). These findings were consistent with an intramucosal adenocarcinoma, developed in a gastric hyperplastic polyp.
Gastric hyperplastic polyps develop as a hyperproliferative response to longstanding inflammation or injury. Although they were originally described as being more common in the gastric antrum (in association with Helicobacter pylori gastritis), they are now known to occur throughout the whole stomach, in particular in autoimmune gastritis. In this setting, hyperplastic polyps represent the most commonly encountered polypoid lesions.
Although essentially benign, these lesions can harbor dysplasia, even high grade dysplasia as documented in our case, which may predispose to gastric cancer and appears to be more frequent in hyperplastic polyps that occur against a background of autoimmune gastritis.
For further reading
Park JY, Cornish TC, Lam-Himlin D, et al. Gastric lesions in patients with autoimmune metaplastic atrophic gastritis (AMAG) in a tertiary care setting.Am J Surg Pathol. 2010 Nov;34(11):1591-1598.
Yamanaka K, Miyatani H, Yoshida Y, et al. Malignant transformation of a gastric hyperplastic polyp in a context of Helicobacter pylori-negative autoimmune gastritis: a case report. BMC Gastroenterol. 2016 Oct 12;16(1):130.
Waldum H, Fossmark R. Gastritis, Gastric Polyps and Gastric Cancer. Int J Mol Sci. 2021 Jun 18;22(12):6548.
Wang Y, Liu Z, Gao W, et al. Malignant transformation of gastric hyperplastic polyps in an autoimmune gastritis patient-a case report and literature review. Front Med. 2025 Oct 23;12:1693184.
Buchner AM, Huang RJ, Lauwers GY, et al. Clinical Practice Update on Management of Gastric Polyps: Expert Review. Clin Gastroenterol Hepatol. 2026 Apr;24(4):893-905.
Presented by
Dr. Ana Lucia Alves, Coimbra, Portugal, and Dr. Cord Langner, Graz, Austria.
